Depending on many different factors in your life, your view of a medical doctor probably varies wildly from your peers. That's even true among medical students. Find one medical student who thinks that doctors should be enriching the lives of their fellow humans and you'll find another who thinks doctors are just workers found in any other banal profession: lawyers, astronomers, sea captains. Which is what makes fourth year so disgusting: there are people who will graduate with me who have terrible ideas on what it means to be human, have no idea what compassion is, and who will probably continue to drive the healthcare machine in this country over a metaphorical cliff into a rift of soul-crushing, human-endangering failure.
Too hyperbolic? Probably. Let me explain:
It really bothers me that there are people who went to medical school because they had a passion for a certain career, and find themselves sending in applications to programs they know they will be denied from because they are terrible applicants. They lack the grades, the board scores, or something as extracurricular as research. They are not.... competitive.
I think dermatology is stupid. I will pick on derm a lot because eyes creep me out and medical imaging was a great advancement, so I optho and radio will be spared my ire in this discussion. The field of dermatology disgusts me because what do dermatologists know that an oncologist (skin cancers) or a well trained primary care physician (rashes) don't? And yet they somehow get paid more for doing less work. It is an artificially competitive field when you compare it to its value in society. And yet some people legitimately like dermatology. The study of skin. I can't fathom why. But they like it--not because they like that there are no emergencies. Not because they will get paid so well and work so little that they will be able to vacation in the fanciest of places atop beautiful yachts. But because they actually like skin and when they see someone with a rash they legitimately want to help them because they see skin as the most important organ of the body. Good hours and ludicrous paychecks are secondary gains--not the prime objective. The prime objective... is people.
And yet this year there will be at least one--from anecdotal evidence--individual who will in all likelihood not match into the field of dermatology despite a strong conviction that that is what they will want to do for the rest of their lives, simply because there are a lot of jackasses out there who see money as the sole solution to all of their ills and who have done so much better on exams that they can and will crowd out the people who would make the best dermatologists.
The best doctors aren't the ones who test best. The best doctors are the ones who are determined to improve the lives of their patients. Studying well and testing well is not the same as staying up late at night worrying how you can implement better care for your patients. Those are two types of hard workers. But only the latter will actually act selflessly whenever possible and improve the lives of others.
Once we start recognizing that--yes--doctors should be smart but they also need to be enthusiastic and deeply invested in their jobs instead of seeing their jobs as a money making venture we can start really making changes to medical machine for the better. For example... why not pay all doctors the same? No matter the field? Remove the pay gaps and see what happens. That would be a fun experiment. It might improve things.
When I was a first year medical student I had an interesting argument with my cousins--who were and continue to be--more conservative than I am. We were discussing healthcare in socialist societies (read: Northern Europe). They were arguing that when you pay doctors not much more than any other profession, you get doctors who really don't want to work hard because there's no point in working harder if you're just going to make the same amount. I actually think this is absolutely wrong. I think if you remove monetary incentives, only the people who actually want to be physicians will become doctors and they will thus work harder because they will love what they do. I think money is great! I love it. And I miss it when I have to spend it on things. But if I knew I would get the same amount of money whether I was an elementary school teacher or a doctor... well I'd still become a doctor because I am really passionate about being a physician. There are things that being a physician provide you that can't be found in other fields to the same degree. There was, and still continues to be although to much lesser a degree, respect for physicians. There is the sense of accomplishment you get from knowing that you know more than most other people. There is the appreciation you receive from patients who will share with you their most intimate of feelings, fears, concerns. My father is a surgeon. He has had the opportunity to be paid a lot of money many times in his life. But he continues to work in inner city Chicago because he enjoys helping people who wouldn't be able to get such surgeries done, even if he knows he will never get paid for operating on them because they have no money, they have no insurance. There were years when my dad made less money from operating than his malpractice insurance cost. That's right--you can make negative money as a physician. But he never considered quitting. Because he has a love for surgery which I don't understand, but which motivates him to work with little consideration to how much money he will make. More physicians should operate (pun intended) in this manner.
I am not an economist. I do not understand the "economy". I simply acknowledge that economic issues must be way more complicated than they appear. Still, just imagine a world where medical school wasn't any more expensive than an undergraduate education. Imagine a world where it was actually free. The person who loves skin diseases--however weird she may be--goes to medical school, falls in love with the study of dermatology, and in her fourth year decides to apply to some dermatology residency programs. Because there are no extrinsic powers enhancing the appeal of dermatology, only those with an intrinsic interest apply. And because skin is such a specific field, much fewer people apply to it. Perhaps the number of applicants correlates with the number of dermatology resident positions available in the field? Dermatology is no more competitive than any other specialty and everyone medical school graduate gets to work in the field they love. They may still not get into their ideal program, but at least they get to be in the OR, or the community, or in the ER, or in a dark room staring at radiographs all day. Which is what they love and want to do well for the rest of their lives.
So what are doctors supposed to be? Well paid or hard working? Money is a great reward for hard work. But it's also a great incentive for people who should not be physicians to enter the field.
I've struggled with how I feel about how much physicians get paid. Honestly, being a medical student, being a resident, and being an attending are all difficult and they should be paid well. But now that I have started to see my friends struggle to get interviews when people who have developed reputations for "getting drunk and beating up people" or "saying really racist things in class" are getting a plethora of invites, I have to question how well this system was set up.
And I will continue to question it. Because money shouldn't drive the motivation for anything. Especially something as important as taking care of people.

Nov 11, 2014
Oct 28, 2014
Money & Politics
So the other day I attended a speech at my medical school entitled "The State of the Medical School Address." I was one of a handful of senior medical students in attendance. The majority of the crowd was a mix of underclassmen--present despite the absence of free food; professors--who looked almost human with their absence of papers and folders and textbooks tucked under their arms; and administrators--eager to be absent from another boring weekday noon meeting.
Overall it was an illuminating presentation. The slides were presented in Prezi, which can make anything look like a Ted Talk, and our school's newly inaugurated Dean, Dr. Tomkoviak, is a psychiatrist so he possessed the appropriate vocabulary and ethos to motivationally interview everyone in attendance--further adding to the Ted Talk vibe. It was nice to hear where our school was going in a suspiciously positive light. But I tried to temper my suspicions with my generally optimistic attitude. It kind of worked, although my cynicism wouldn't completely shut off. Chicago has many highly ranked medical schools and despite being The Chicago Medical School it is hard to stand out and be exceptional. We were also placed on probation by the LCME, as well. Another insult and another reason to wonder if this speech wasn't just a publicity stunt filled with half-truths and full lies.
Our dean talked about what he would be doing as our leader. Essentially he vowed to help everyone work together, allowing the staff and the students to work towards a similar vision of excellence. At times it almost sounded as though he would start telling us that we were "poised to shift paradigms by synergizing our individual strengths" -- it was one of those kind of talks that seemed displaced from the 1980s. I tried not to roll my eyes or laugh. I stayed optimistic.
Finally he mentioned some highlights of the work our administrators were doing for the good of the students, important additions to our school's plan: the creation of more residency programs affiliated with our school and the creation of a 5th year program for those students who fail to match, two wonderful additions for future graduates. He also talked about finding more clinical opportunities for students. All wonderful things. This part of the talk I didn't roll my eyes, I didn't scoff. I was in awe. I was grateful.
But in the end I found two things deeply upsetting. The first was the almost complete omission of our outrageous tuition. At almost 60k a year it's no wonder our school has struggled with diversifying our student population in recent years, a problem which the LCME noticed and used to place us on probation, along with the high debt among graduating students. Our tuition is the most expensive in Illinois--even more than Northwestern's medical school, whose students purportedly are given rental cars to commute to clinical rotations lest they lack a car of their own. A diverse student population is something our school has always been committed to, even from its start in 1912. Something that no other medical school still standing in Illinois today can claim. But how can we ask people--even the most driven among them--to jump into nearly a quarter of a million dollars in debt? That's insane. This shouldn't be happening. And even though, sadly, escalating student debt is not a unique problem to Chicago Medical School, I think students of our school should know exactly why our tuition is so high. What are we paying for? If it's the renovated and lovely cafeteria that closes absurdly early at 2 PM, I hate to say this... but I think we could have made do without. As somebody who's been well briefed about the political corruption in the City of Chicago, I can't believe that any entity with 'Chicago' in its title is free of any monetary mismanagement. Where's our money going? Understandably to hospitals and professors--for our education. For standardized patients and to purchasing online scholarly journals--also for our education. But I can't believe with a class size of almost 200 students (and at 60k a year that's roughly 12 million dollars in revenue), all that money is being used wisely. Where's the waste? What can we do about it?
Which leads me to the way the speech ended and the second thing that ticked me off. During the talk, the dean mentioned a new twitter campaign and offered a prize to a randomly drawn tweeter using the hashtag #CMSPLEDGE. Social media at its finest! The winner was a medical student. The dean proudly handed her a gift bag and asked her to open it. She pulled out an IPAD mini. To help her with her studies in the evolving world of medical education. A nice symbolic gesture. And a nice gift. Almost as an aside he mentioned: "And to all of you students wondering, I didn't use any of your tuition money to buy this. I paid for that myself." A comment that garnered many laughs. Yet I was outraged. Sure our tuition money didn't go directly into buying gifts. That would be--and the only course I ever failed was accounting so I'm sure I'll mess this up but--that would be some form of money laundering, right? Regardless, it has been proposed that one of the causes for the ever increasing cost of higher education is the money paid to top administrators. Like deans. Like CEOs. Like non-essential and inept staff who don't respond to your emails on time and who belittle you once they finally respond to your originally non-urgent but now emergent requests because it was sitting, neglected, in an inbox for three weeks. Okay, so not so much that last one. But that's an inefficiency all the same. And if the CEO of our university is making $500,000 dollars a year for essentially being a figurehead, I've got to ask if that money would be better used to give eight to ten medical students 100% tuition assistance.
I'm not claiming to know anything about business models or how to run a university. But I do know that in some small way my peers and I helped pay for that IPAD mini and I would much rather have had assistance paying for any number of the many additional fees of medical school few people tell you about.
I love my school. The students represent--in my personal and likely biased opinion--some of the most hardworking and honest medical students you can find in Chicago. And whether or not it was motivated by being placed on probation, I like the way our school keeps thinking up innovative changes to the curricula. Our school has emphasized liberal arts to the long term benefit of every one of its graduates. And I appreciate that. I truly due. But the fact that tuition wasn't addressed heavily tells me that either it was too difficult or too depressing of a topic to put into a motivating speech or that nobody at the top cares about this specific problem. And if tuition isn't seriously addressed, I fear that the quality of the CMS graduate will decline not because of any weaknesses in the school's academics, but because it will be admitting only those students who can look at a quarter million dollar pricetag and not flinch.
Overall it was an illuminating presentation. The slides were presented in Prezi, which can make anything look like a Ted Talk, and our school's newly inaugurated Dean, Dr. Tomkoviak, is a psychiatrist so he possessed the appropriate vocabulary and ethos to motivationally interview everyone in attendance--further adding to the Ted Talk vibe. It was nice to hear where our school was going in a suspiciously positive light. But I tried to temper my suspicions with my generally optimistic attitude. It kind of worked, although my cynicism wouldn't completely shut off. Chicago has many highly ranked medical schools and despite being The Chicago Medical School it is hard to stand out and be exceptional. We were also placed on probation by the LCME, as well. Another insult and another reason to wonder if this speech wasn't just a publicity stunt filled with half-truths and full lies.
Our dean talked about what he would be doing as our leader. Essentially he vowed to help everyone work together, allowing the staff and the students to work towards a similar vision of excellence. At times it almost sounded as though he would start telling us that we were "poised to shift paradigms by synergizing our individual strengths" -- it was one of those kind of talks that seemed displaced from the 1980s. I tried not to roll my eyes or laugh. I stayed optimistic.
Finally he mentioned some highlights of the work our administrators were doing for the good of the students, important additions to our school's plan: the creation of more residency programs affiliated with our school and the creation of a 5th year program for those students who fail to match, two wonderful additions for future graduates. He also talked about finding more clinical opportunities for students. All wonderful things. This part of the talk I didn't roll my eyes, I didn't scoff. I was in awe. I was grateful.
But in the end I found two things deeply upsetting. The first was the almost complete omission of our outrageous tuition. At almost 60k a year it's no wonder our school has struggled with diversifying our student population in recent years, a problem which the LCME noticed and used to place us on probation, along with the high debt among graduating students. Our tuition is the most expensive in Illinois--even more than Northwestern's medical school, whose students purportedly are given rental cars to commute to clinical rotations lest they lack a car of their own. A diverse student population is something our school has always been committed to, even from its start in 1912. Something that no other medical school still standing in Illinois today can claim. But how can we ask people--even the most driven among them--to jump into nearly a quarter of a million dollars in debt? That's insane. This shouldn't be happening. And even though, sadly, escalating student debt is not a unique problem to Chicago Medical School, I think students of our school should know exactly why our tuition is so high. What are we paying for? If it's the renovated and lovely cafeteria that closes absurdly early at 2 PM, I hate to say this... but I think we could have made do without. As somebody who's been well briefed about the political corruption in the City of Chicago, I can't believe that any entity with 'Chicago' in its title is free of any monetary mismanagement. Where's our money going? Understandably to hospitals and professors--for our education. For standardized patients and to purchasing online scholarly journals--also for our education. But I can't believe with a class size of almost 200 students (and at 60k a year that's roughly 12 million dollars in revenue), all that money is being used wisely. Where's the waste? What can we do about it?
Which leads me to the way the speech ended and the second thing that ticked me off. During the talk, the dean mentioned a new twitter campaign and offered a prize to a randomly drawn tweeter using the hashtag #CMSPLEDGE. Social media at its finest! The winner was a medical student. The dean proudly handed her a gift bag and asked her to open it. She pulled out an IPAD mini. To help her with her studies in the evolving world of medical education. A nice symbolic gesture. And a nice gift. Almost as an aside he mentioned: "And to all of you students wondering, I didn't use any of your tuition money to buy this. I paid for that myself." A comment that garnered many laughs. Yet I was outraged. Sure our tuition money didn't go directly into buying gifts. That would be--and the only course I ever failed was accounting so I'm sure I'll mess this up but--that would be some form of money laundering, right? Regardless, it has been proposed that one of the causes for the ever increasing cost of higher education is the money paid to top administrators. Like deans. Like CEOs. Like non-essential and inept staff who don't respond to your emails on time and who belittle you once they finally respond to your originally non-urgent but now emergent requests because it was sitting, neglected, in an inbox for three weeks. Okay, so not so much that last one. But that's an inefficiency all the same. And if the CEO of our university is making $500,000 dollars a year for essentially being a figurehead, I've got to ask if that money would be better used to give eight to ten medical students 100% tuition assistance.
I'm not claiming to know anything about business models or how to run a university. But I do know that in some small way my peers and I helped pay for that IPAD mini and I would much rather have had assistance paying for any number of the many additional fees of medical school few people tell you about.
I love my school. The students represent--in my personal and likely biased opinion--some of the most hardworking and honest medical students you can find in Chicago. And whether or not it was motivated by being placed on probation, I like the way our school keeps thinking up innovative changes to the curricula. Our school has emphasized liberal arts to the long term benefit of every one of its graduates. And I appreciate that. I truly due. But the fact that tuition wasn't addressed heavily tells me that either it was too difficult or too depressing of a topic to put into a motivating speech or that nobody at the top cares about this specific problem. And if tuition isn't seriously addressed, I fear that the quality of the CMS graduate will decline not because of any weaknesses in the school's academics, but because it will be admitting only those students who can look at a quarter million dollar pricetag and not flinch.
Oct 7, 2014
Hospital Billing and Insurance
The prompt for this next clinical reflection meeting at school was the following: To what extent are physicians' values and decisions responsible for the cost of health care, and what responsibility do we have to control costs? How cost-conscious have the physicians you have worked with been, and what rolled does financial stewardship have in the professional responsibilities of physicians?
But like so many other things, I was still angry about dropping $175 at Walgreens the other day for 3 vials of lantus and two boxes of test strips, so I had trouble focusing:
I think it is fundamentally irresponsible to be a
physician unaware of the costs of medicine and health care services. That being
said, a lot of physicians don't want to worry themselves with the details. Have
I ever worked with a physician who seemed to understand how much things cost
for patients? Not really. No. But consider this: how many physicians actually
have chronic illnesses? How many doctors are on a ton of prescriptions at any
one time?
Sep 14, 2014
On the Eve of ERAS (applying to residency programs)
I'm on the floor with my head cradled into my pillow. I'm dragging in slow but shallow breaths, smelling the scent of leave-in hair conditioner that has diffused into the pillow cover since last washing it several weeks ago.
There's a bottle of extra strength Excedrin and a bottle of antacids sitting on the table that I was previously sitting at. They've done nothing. My head hurts and my stomach hurts and I don't know why. Or rather, I either gave myself food poisoning via homemade balsamic vinaigrette for a delicious salad eaten midday or I am so stressed out that my body is forcing me to give up on what was previously a fun challenge:
Write the Great American Personal Statement.
I believe my psychogenic pain is telling me it's impossible.
Tomorrow I will have to submit 28 to 30 applications (depending on if I delete/add any new programs in the next 24 hours) to family medicine residency programs that are literally all around the country. Or maybe I'll splurge and apply to 75 programs, like some people I know who are applying to more difficult specialties. They will shell out more than $3,000. But the common motto is: "It's cheaper than having to apply next year." Implying that many of us won't get interviews and ultimately match unless we apply far and wide and broadly because we're.... what? Not motivated? Not dedicated? Not humane? No the answer is "less competitive." But what the hell is competitive? I don't know. I really don't. It's different for every specialty and every program within that specialty.
Each application will include a copy of my personal statement. The Great American Personal Statement.
Oh hell. And then there's the added anxiety that is trying to end up in the same location as my significant other who is also going to attempt to match this year. The likelihood of us matching in the same geographic location is so... unlikely that honestly we should probably just break-up right now and stop prolonging a fantasy that is doomed to fail.
Unless I can write the Great American Personal Statement.
Because then maybe I'll get interviews everywhere.
And then all my dreams will come true. I'll become an awesome resident who will have an awesome career, and despite it being "impossible" to have a private practice, I will have one. I will have it all.
But literally, only if I write the Great American Personal Statement.
So I'm whimpering through and over-analyzing every sentence, every paragraph, every idea, every phrase. This is impossible. Everything's impossible. What is medicine? Why am I doing this?
Because I'm a smart young adult willing to dedicate my life to years like this last one. With days like this one. Spent over analyzing the smallest of details. Because I want to improve the lives of those around me. Because I want to serve communities in a way that will make lives healthier, happier, and more productive.
Because I want to be happy with the life I've lived. I want to die knowing that what I have accomplished has made a difference in this world, if only for a moment in the grand scheme of things. But that I've effected change. That I've made others happy.
Oh my god. I'm crying. I'm literally crying right now. Because all I want is to help people. Which sounds so stupid and has been said so many goddamn times. But it's true. Why can't I just write that? Why can't I just put that in my personal statement? The Great f***ing American Personal Statement. I want to help people. My name is Elora Apantaku and I will literally do everything I can to help people until the day I die.
There's a bottle of extra strength Excedrin and a bottle of antacids sitting on the table that I was previously sitting at. They've done nothing. My head hurts and my stomach hurts and I don't know why. Or rather, I either gave myself food poisoning via homemade balsamic vinaigrette for a delicious salad eaten midday or I am so stressed out that my body is forcing me to give up on what was previously a fun challenge:
Write the Great American Personal Statement.
I believe my psychogenic pain is telling me it's impossible.
Tomorrow I will have to submit 28 to 30 applications (depending on if I delete/add any new programs in the next 24 hours) to family medicine residency programs that are literally all around the country. Or maybe I'll splurge and apply to 75 programs, like some people I know who are applying to more difficult specialties. They will shell out more than $3,000. But the common motto is: "It's cheaper than having to apply next year." Implying that many of us won't get interviews and ultimately match unless we apply far and wide and broadly because we're.... what? Not motivated? Not dedicated? Not humane? No the answer is "less competitive." But what the hell is competitive? I don't know. I really don't. It's different for every specialty and every program within that specialty.
Each application will include a copy of my personal statement. The Great American Personal Statement.
Oh hell. And then there's the added anxiety that is trying to end up in the same location as my significant other who is also going to attempt to match this year. The likelihood of us matching in the same geographic location is so... unlikely that honestly we should probably just break-up right now and stop prolonging a fantasy that is doomed to fail.
Unless I can write the Great American Personal Statement.
Because then maybe I'll get interviews everywhere.
And then all my dreams will come true. I'll become an awesome resident who will have an awesome career, and despite it being "impossible" to have a private practice, I will have one. I will have it all.
But literally, only if I write the Great American Personal Statement.
So I'm whimpering through and over-analyzing every sentence, every paragraph, every idea, every phrase. This is impossible. Everything's impossible. What is medicine? Why am I doing this?
Because I'm a smart young adult willing to dedicate my life to years like this last one. With days like this one. Spent over analyzing the smallest of details. Because I want to improve the lives of those around me. Because I want to serve communities in a way that will make lives healthier, happier, and more productive.
Because I want to be happy with the life I've lived. I want to die knowing that what I have accomplished has made a difference in this world, if only for a moment in the grand scheme of things. But that I've effected change. That I've made others happy.
Oh my god. I'm crying. I'm literally crying right now. Because all I want is to help people. Which sounds so stupid and has been said so many goddamn times. But it's true. Why can't I just write that? Why can't I just put that in my personal statement? The Great f***ing American Personal Statement. I want to help people. My name is Elora Apantaku and I will literally do everything I can to help people until the day I die.
Aug 30, 2014
Socially Valuable
"Remember that competitiveness does not equate to what is rewarding or socially valuable. The least competitive specialties, Family Medicine and Internal Medicine, are highly rewarding and are perhaps in the greatest social demand." - Dean of Students in an E-mail to fourth year students
Aug 27, 2014
A comment from an article from io9.com: "The Herd Mentality of the Anti-Vaxxer Movement"
Pediatrician: Will you be vaccinating your children?
Parent: No.
Pediatrician: Please leave my office.
He then goes on to explain himself -
I often wonder why a parent who believes vaccines are harmful would want to bring their children to a medical doctor at all. After all, for immunizations to be as malign as their detractors claim, my colleagues and I would have to be staggeringly incompetent, negligent or malicious to keep administering them.
If vaccines caused the harms Jenny McCarthy and her ilk claim they do, then my persistence in giving them must say something horrifying about me. Why would you then want to bring your children to me when you're worried about their illnesses? As a parent myself, I wouldn't trust my children's care to someone I secretly thought was a fool or a monster.
Pediatrician: Will you be vaccinating your children?
Parent: No.
Pediatrician: Please leave my office.
He then goes on to explain himself -
I often wonder why a parent who believes vaccines are harmful would want to bring their children to a medical doctor at all. After all, for immunizations to be as malign as their detractors claim, my colleagues and I would have to be staggeringly incompetent, negligent or malicious to keep administering them.
If vaccines caused the harms Jenny McCarthy and her ilk claim they do, then my persistence in giving them must say something horrifying about me. Why would you then want to bring your children to me when you're worried about their illnesses? As a parent myself, I wouldn't trust my children's care to someone I secretly thought was a fool or a monster.
probably something guys don't have to think about
While I was at the National Conference for Family Physicians, I had the opportunity to walk around and meet residents from over 400 family medicine residency programs. It was... awkward.
I am a socially awkward person. Put me in a room of a 1000+ people who I have to present my best features to and well... yea. Not so much fun.
But definitely interesting. I remarked to someone that had this been a conference for any other type of physician and I would probably be crying in a corner. Family practitioners are usually pretty funny or at least try to appear friendly. So that's.... something to comfort the social anxiety.
A strange thought occurred, however, when I was talking at length about a program with one resident. I think he was flirting with me. Which would be inappropriate so he probably wasn't... but what if he was? I mean--I'm also terrible at telling if a person is attracted to me and everyone was earnestly trying to be friendly. My face always hurt from awkward smiling once I returned to my hotel room. But seriously... what if he was? Could I use that? Could I take advantage of that to get into a residency program?
Sick, right?
Strange.
This is probably something most guys don't have to think about.
I am a socially awkward person. Put me in a room of a 1000+ people who I have to present my best features to and well... yea. Not so much fun.
But definitely interesting. I remarked to someone that had this been a conference for any other type of physician and I would probably be crying in a corner. Family practitioners are usually pretty funny or at least try to appear friendly. So that's.... something to comfort the social anxiety.
A strange thought occurred, however, when I was talking at length about a program with one resident. I think he was flirting with me. Which would be inappropriate so he probably wasn't... but what if he was? I mean--I'm also terrible at telling if a person is attracted to me and everyone was earnestly trying to be friendly. My face always hurt from awkward smiling once I returned to my hotel room. But seriously... what if he was? Could I use that? Could I take advantage of that to get into a residency program?
Sick, right?
Strange.
This is probably something most guys don't have to think about.
Aug 25, 2014
Brainwash 'n Vent
There it was. The truth. Stretched out in front of me like the end of days. And loudness. So much strife and bustle. Everywhere. Cars and the people with their voices and the humming of buildings with their AC units pumping in cold to isolated rooms separated from the world and the streets within the city of Chicago. And the El up ahead a block, three or four stories high with always the same voice alerting passengers and future passengers alike: "Doors opening." Then two bells. Then: "Doors closing." This was my present but less than an hour ago I was in a completely different world. Oppressive silence. The distant sounds of mouses being clicked at other terminals was the only thing to distract the dull buzz that came with inactive listening from taking hold on my ears. Distant, fluorescent lights. Everything controlled. And cold. So cold. That was the world of the United States Medical Licensing Examination Step 2, the second of three licensing exams. And I realized on the streets of Chicago, I could not remember a single question. 355 questions. 9 hours. And I couldn't remember a single thing.
What could possibly be more horrifying?
Step 2 is a serious exam, of course, otherwise, why would we have to pay $580 to take it? If cost equals quality, then Step 2 is a lot more important than the scantrons and blue notebooks I used to use in high school to take advanced placement (AP) exams--which actually helped me take less courses in college, saving me thousands of dollars. I think those cost $25. USMLE tests cost me money to prove that I can be a doctor. I guess if failed enough times, I would have to take a year of medical school again: $50,000. Okay.
AP scores can be dolled out in a simple 1, 2, 3, 4, or 5. Step scores are much much much more complicated. Not always was this so, of course. In the old days, you passed or you failed. Quite simple really. Because we all must be evaluated and found worthy of the MD that will follow our names for the rest of our lives, but do 355 randomly selected and sometimes silly questions mean that we deserve or do not deserve to put our hands on a patient, to share in their suffering, to help and to heal and to comfort and advise? No. They really, honestly shouldn't.
This year the passing score on Step 2 jumped up from 200 to 209. Was this arbitrary? How was this determined? And isn't nine points.... a lot of points? More importantly, if the passing grade was just determined based on how many people passed Step 2--which is the way some courses are run-- wouldn't this imply some kind of insidious ploy to make sure that enough people fail so that the administrators of USMLE can charge some poor soul another $580 and increase revenue? Or does the increased score make everyone feel better that residents are intelligent enough to be able to control and manage possibly dying patients, and the additional money made is just an extra benefit?
How many times have I heard a discouraged patient say something along the lines of, "I know you just see me as money to be made at my expense." Should I also feel the same way, as a medical student, stuck in a world of constant cost with no monetary profit?
Let's assume however, that a lot of thought was made into making it so that 209 was meant to really pick out who would do well as a resident in terms of knowledge. Isn't it possible that there are people who score below 209 who would make good residents because they know how to look up answers on uptodate or even google? And who work hard to make sure that they overcome their deficits? Conversely, couldn't someone with above a 209 simply make the worst resident ever and incur a lot of lawsuits because of they have the worst bedside manner? Or couldn't someone with a +209 score completely slack off for the rest of their career and be unable to provide the standards of care for anyone besides the hypothetical patients he saw before him in paragraphs on a computer screen on test day? I mean statistically, some people who score below 209 will ultimately practice great medicine while people who score above 209 will do absolutely terrible things.
So did I really need to be locked in a room for 9 hours--an amnesia-inducing, cubicle-filled room with no music, no food, no human contact for 9 hours--so that I could answer 355 questions that I would instantly forget and then spend the next three weeks until receiving my score panicking and scratching at my skin, picking at my scabs, and eating antacids like candy because how can you feel like you did well on a test if you can't remember any part of it? Only to find out that I did pass and that I did do well.
All that nervousness and I have to pay $580. Infuriating.
What could possibly be more horrifying?
Step 2 is a serious exam, of course, otherwise, why would we have to pay $580 to take it? If cost equals quality, then Step 2 is a lot more important than the scantrons and blue notebooks I used to use in high school to take advanced placement (AP) exams--which actually helped me take less courses in college, saving me thousands of dollars. I think those cost $25. USMLE tests cost me money to prove that I can be a doctor. I guess if failed enough times, I would have to take a year of medical school again: $50,000. Okay.
AP scores can be dolled out in a simple 1, 2, 3, 4, or 5. Step scores are much much much more complicated. Not always was this so, of course. In the old days, you passed or you failed. Quite simple really. Because we all must be evaluated and found worthy of the MD that will follow our names for the rest of our lives, but do 355 randomly selected and sometimes silly questions mean that we deserve or do not deserve to put our hands on a patient, to share in their suffering, to help and to heal and to comfort and advise? No. They really, honestly shouldn't.
This year the passing score on Step 2 jumped up from 200 to 209. Was this arbitrary? How was this determined? And isn't nine points.... a lot of points? More importantly, if the passing grade was just determined based on how many people passed Step 2--which is the way some courses are run-- wouldn't this imply some kind of insidious ploy to make sure that enough people fail so that the administrators of USMLE can charge some poor soul another $580 and increase revenue? Or does the increased score make everyone feel better that residents are intelligent enough to be able to control and manage possibly dying patients, and the additional money made is just an extra benefit?
How many times have I heard a discouraged patient say something along the lines of, "I know you just see me as money to be made at my expense." Should I also feel the same way, as a medical student, stuck in a world of constant cost with no monetary profit?
Let's assume however, that a lot of thought was made into making it so that 209 was meant to really pick out who would do well as a resident in terms of knowledge. Isn't it possible that there are people who score below 209 who would make good residents because they know how to look up answers on uptodate or even google? And who work hard to make sure that they overcome their deficits? Conversely, couldn't someone with above a 209 simply make the worst resident ever and incur a lot of lawsuits because of they have the worst bedside manner? Or couldn't someone with a +209 score completely slack off for the rest of their career and be unable to provide the standards of care for anyone besides the hypothetical patients he saw before him in paragraphs on a computer screen on test day? I mean statistically, some people who score below 209 will ultimately practice great medicine while people who score above 209 will do absolutely terrible things.
So did I really need to be locked in a room for 9 hours--an amnesia-inducing, cubicle-filled room with no music, no food, no human contact for 9 hours--so that I could answer 355 questions that I would instantly forget and then spend the next three weeks until receiving my score panicking and scratching at my skin, picking at my scabs, and eating antacids like candy because how can you feel like you did well on a test if you can't remember any part of it? Only to find out that I did pass and that I did do well.
All that nervousness and I have to pay $580. Infuriating.
Aug 14, 2014
Family Medicine Conference
Last weekend I drove eight hours to Kansas City, Missouri for a national conference for residents and medical students in and interested in family medicine. My specialty adviser suggested I go since almost all of the residency programs in the United States set up booths to interest and inform students. I require a few more weeks of electives in the year, and it was her hope (and mine, too, although I am always much less optimistic about my ability to socialize and form plans with strangers than most people who know me) that I'd be able to establish some sort of elective in rural medicine there.
I did not.
All totaled, the weekend cost me around $800 - $900. But I would have gone back if I had the choice, because despite being really draining to walk among so many strangers constantly, it was really inspiring. I feel really inspired. I have felt this way previously at the end of AMWA conferences, so I can only assume I love conferences more than I love school.
The lecturers were phenomenal. They were so passionate. And so funny. And so personable and nice. After spending a year interacting with doctors who seemed dissatisfied with their career choices, it was nice to see people loving what they did.
And everyone spoke in such a way as to relate several main themes:
1. Many physicians think family medicine is a joke but that is slowly changing.
2. There's a lot of good you can do as a family physician--be it for your patients or even in changing politics.
3. Job satisfaction. Family practitioners have more of it.
There were more ideas but I've started having a hard time writing anything of importance. More to follow.
I did not.
All totaled, the weekend cost me around $800 - $900. But I would have gone back if I had the choice, because despite being really draining to walk among so many strangers constantly, it was really inspiring. I feel really inspired. I have felt this way previously at the end of AMWA conferences, so I can only assume I love conferences more than I love school.
The lecturers were phenomenal. They were so passionate. And so funny. And so personable and nice. After spending a year interacting with doctors who seemed dissatisfied with their career choices, it was nice to see people loving what they did.
And everyone spoke in such a way as to relate several main themes:
1. Many physicians think family medicine is a joke but that is slowly changing.
2. There's a lot of good you can do as a family physician--be it for your patients or even in changing politics.
3. Job satisfaction. Family practitioners have more of it.
There were more ideas but I've started having a hard time writing anything of importance. More to follow.
Jul 25, 2014
A Scribbled Story on the back of my Ob/Gyn Orientation Packet
The woman was clutching her left shoulder with her right hand. Intermittently, as she spoke, she would press against it, as though she could fix her heart by coaxing the arm into a well-massaged, relaxed and quiescent state. Her skin was loose and wrinkled, falling away from her hands, her arms, her face, her bones that were most likely thinned out and brittle. Despite drowning in her own skin, she looked her stated age of 82. Maybe even a few years younger. I had originally approached her and let my crossed arms lay on the railing that had been pulled up from her emergency room bed. But regardless of my physical closeness and what many have told me is a great bed side manner, the woman did not warm up to me initially. She was serious. She had a serious complaint, of course, otherwise why bother taking a day off work going to the emergency room. She would later tell me that she worked as a Walmart cashier. She loved working there, being surrounded by people. She didn't want this job--this world--to be taken away from her because she didn't take the warning signs of a heart attack seriously.
- true story from my emergency medicine rotation -
Jul 23, 2014
Assumed, Actual, and Average Performance: Preparing for the horrors of Step 2 using the defense mechanism of Intellectualization
In exactly one week (7 days -- 168 hours -- 10,080 minutes -- you get the idea) I will be sitting in a prometric testing center taking, depending on whom you talk to, the most important test I have ever taken capable of determining all of my future career successes, or just something I need to pass to graduate: The United States Medical Licensing Examination (USMLE) Step 2 Clinical Knowledge.
Tensions are running high, but I am actually quite proud of myself. I began studying weeks, no... months ago, and I find that even though I only have a week left, I am doing a lot less cramming than I had to do for Step 1. And I actually might finish reading an entire review book cover to cover. I may actually do well on this exam.
But do you know what's more important than doing well on exams? Knowing, fairly accurately when you leave the testing center, that you have most likely passed the exam with a 95% confidence interval (did I use that term correctly? I still haven't studied biostatistics). Which is why I have begun analyzing my Usmleworld QBank tests. Upon hitting submit, I quietly contemplate how well I think I may have done, remembering how many questions I "knew" verse how many were "good guesses" verse the inevitable "I have narrowed it down to two, equally likely choices" verse "I have not heard of any of these conditions. I will choose the answer choice that seems most viable." Then I write down my assumed score. Then I write down my actual score and the national average for those 44 questions.
What conclusions have I come to? First, my actual performance varies widely. Hopefully over my next tests I can become more consistent, although this isn't likely. I believe this is the nature of any test designed to ask many questions on broad topics.
Second, my predictions are much more conservative than my actual performances. Which is nice to know, although a given: more people feel like they failed an exam than actually did, at least in medical school.
Third, my predictions seem to follow my actual scores fairly closely, although doing really well on test 94 improved my confidence so that on test 95, I assumed I did much better -- even though I in fact did much worse.
And now I have to study for at least six more hours before I can go to sleep. I love summer break.
Tensions are running high, but I am actually quite proud of myself. I began studying weeks, no... months ago, and I find that even though I only have a week left, I am doing a lot less cramming than I had to do for Step 1. And I actually might finish reading an entire review book cover to cover. I may actually do well on this exam.
But do you know what's more important than doing well on exams? Knowing, fairly accurately when you leave the testing center, that you have most likely passed the exam with a 95% confidence interval (did I use that term correctly? I still haven't studied biostatistics). Which is why I have begun analyzing my Usmleworld QBank tests. Upon hitting submit, I quietly contemplate how well I think I may have done, remembering how many questions I "knew" verse how many were "good guesses" verse the inevitable "I have narrowed it down to two, equally likely choices" verse "I have not heard of any of these conditions. I will choose the answer choice that seems most viable." Then I write down my assumed score. Then I write down my actual score and the national average for those 44 questions.
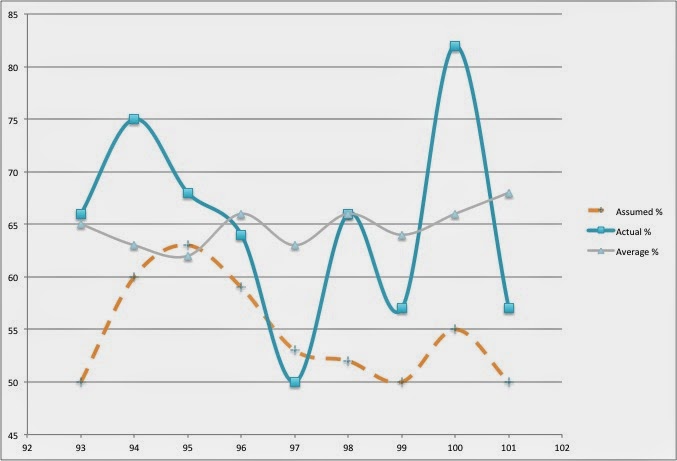 |
| Test Results of QBank tests numbers 93 through 101 |
Second, my predictions are much more conservative than my actual performances. Which is nice to know, although a given: more people feel like they failed an exam than actually did, at least in medical school.
Third, my predictions seem to follow my actual scores fairly closely, although doing really well on test 94 improved my confidence so that on test 95, I assumed I did much better -- even though I in fact did much worse.
And now I have to study for at least six more hours before I can go to sleep. I love summer break.
Jul 9, 2014
"Unique Opportunity" for the PCP (i.e., psychotherapy)
"Primary care practitioners have a unique opportunity to address the emotional needs of their patients, but regardless of their importance, these needs must be handled in a time-effective manner. The psychosocial aspect of patients' problems must be effectively addressed within the regular 10 or 15-minute medical visit. The therapeutic goal is to help patients reorganize some small aspect of their self-concept or behavior in a more comfortable, productive, or, at minimum, less destructive manner. The healing grows out of the established practitioner-patient relationship."
Stuart MR, Lieberman JA III. The Fifteen Minute Hour: Therapeutic Talk in Primary Care. United Kingdom, Oxon: Radcliffe Publishing Ltd.; 2008.
Very interesting thought. And I suppose, a good goal for someone like me who--if I ever become comfortable enough with it--would spend much more than 10 - 15 minutes on therapy with a patient.
Jun 30, 2014
Social Phobia
My step 2 studying attempts are progressing nicely (mostly thanks to habitrpg.com, which allows me to incentivize my daily study habits and my lengthy to-do list).Did I know that I meet the criteria for having both social and specific phobias? No!
My friends and I went out to dinner tonight and we mutually commiserated on how awful studying for huge tests is. But I really think studying for step 1 was worse. I have terrible flashbacks of skin flaking off of my face and my ears bleeding.
Step 2 is better if only because it is more interesting:
Although it makes sense. As much as I love talking to patients, I dread actually introducing myself to people. I frequently find that I yell at myself for missing an opportunity to talk to a stranger, or engage with a patient longer. Little things will bother me for the rest of the day, like when I missed an opportunity to say thank you to someone at the park who helped me figure out how to work the water fountain.
The treatment for social phobias is cognitive behavioral therapy (CBT) and SSRIs.
Cognitive behavioral therapy really fascinates me, but I think that's mostly because it's always listed as an efficacious treatment for many psychiatric disorders which I think is pretty counter-intuitive. Psychiatrists (they can prescribe you drugs because they are doctors) are thought of as superior to clinical psychologists (they can talk to you because they are Ph.D's), yet both medicating and therapy are equally effective for a lot of mood and anxiety disorders.
Regardless, I guess I could start trying to enforce CBT on myself. I could assess why I avoid talking to strangers and how that behavior is affecting my life. I could try to change it. I could slowly mold myself to become the person I've always wanted to be--gregarious, friendly, fun--using various tricks I've found on the internet or in self-help books.
On the other hand, I could just ask my psychiatrist to switch me to an SSRI.
Jun 5, 2014
Out of Bounds
I’ve never been a huge
fan of babies. Toddlers are cute and "children are our future", but neonates are
really boring. In comparison with other newborns of the mammalian order, human
babies are completely useless. Utterly useless… 30 days in and they can only
coo? And they don’t start speaking intelligible words for at least 270 days?
Not impressed.
But several weeks ago, a
patient on the floor was a five month old and she was puffy-cheeked, bright-eyed, and adorable. A complicated
perinatal period had ensured that she would require intensive additional medical
attention indefinitely, and now she was back in the hospital with r/o aspiration pneumonia
after a two week reprieve at home.
At five months of age, she was
operating at a one to two month old level. There was no social smile, no
babbling of words, no raking grasp. But she was able to grip my pointer finger
whenever I placed it near her palm, and I thought that was a good sign. I spent
a lot of time with this baby. Partially because I was trying to figure out what milestones she had missed as a way of quizzing myself on infant behavior, but mostly because she was adorable.
And I never saw the
parents. For an entire week I watched this baby--rotating her head to help her
plagiocephaly; baby talking at her so she could hear words; setting her on her stomach for tummy time to develop motor skills; smiling into her
face so she could see facial expressions. And I never once saw the parents.
I checked in her files to
figure out her family story. Several young children at home, maybe they weren’t
ignoring her. Maybe they weren’t bad parents.
But I still worried. It’s
weird how attached one can be to a thing that never smiles. And I wanted to
guarantee her safety. I wanted to tell people about my frustrations and my
fears for how this baby might grow up. But who would I tell? And in a hospital full of sick kids, was this kid any more special than anyone else?
Yes. Of course. She was my patient. I was her hospital guardian. Every minute of free time I had on the wards I'd gown up, put my gloves on, and hold her hand while I tried to get her to smile.
Miraculously, somehow, I
finally met the parents. Or rather, the patient did. They were a flurry of
excitement as they entered the room, mother and father and brother. And
suddenly her face was being kissed and her mother was pulling out tiny matching outfits from a shopping bag for her to try on before she was discharged home.
I was fortunate this
time. This baby was going to be a burden on this family--no question. But this family had a lot of something that I wish I had seen more of as a child: love. I no longer felt a need to voice my concerns. But I wonder how distant I’ll
be able to keep myself the next time I see a patient in need of more than just
medical care.
Apr 29, 2014
Dream Office #2
It would be nice if the first time you saw your doctor, the doctor took your vitals themselves. Traditionally nurses or other office workers take down your measurements, and while this is incredibly efficient, it probably makes people feel as if they are being processed.
Apr 13, 2014
Planning the Rest of Your Life
It happened when I was being active in the milieu, playing bananagrams with a handful of occupants admitted to the in-patient psych ward: two suicide attempts, one recurring major depressive disorder not responding to recent medication changes, and a non-psychotic manic depressive who in conversation appeared to be slightly more psychotic than the notes suggested. I was rather enjoying myself, realizing that I could spend hours talking to any one of these people. The etiology of mood disorders had always fascinated me, and now I was able to explore them by myself, at my leisure.
And although these patients were very kind and open, they were growing frustrated with another patient--a schizoaffective--roaming the common area: she would not stop talking. It wasn't pressured speech--it was continuous speech. It was rambling, non-directed speech, spoken to the hospital at large, and it was spoken with an annoying twangy accent that could be described as an inner city uptown chicago accent--very short A's.
The bananagram players began to mock her, not to her face, but they began to mimic her monologues as they spelled out intersecting words. Halfway through the game, one of my patients, a very irritable and consistently antagonizing schizophrenic, sat down at our table and tried to get on my nerves, insulting just about everything he could get his mind to focus on. The guise of bananagrams saved me because I appeared and actually was busy, trying to win a game. He left shortly and I felt relieved to once again be surrounded only by the moods. And I realized, painfully, that I could not go into psychiatry. I loved my mood disorder patients, but I couldn't tolerate the psychotic ones for more than a few minutes. And while I could eventually work solely outpatient and see only patients with predominantly mood disorders, psychiatry residency programs are four years long, so I'd be spending four years doing something I could kind of tolerate to do something I'd probably love for the rest of my life.
As a third year nearing the end of her clerkship rotations, I've been spending a disturbing amount of time freaking out--I suppose the correct term would be "having panic attacks"--about my future. But my debate between family medicine and psychiatry is far simpler than some of my friends considering even longer residency programs.
Take my good friend Annette. Everything about her screams surgeon: her steady, unshakable confidence, her ability to immediately befriend and then joke-around with just about anyone, her oversized-for-her-stature-hands. Surgeon! But if she was to become a surgeon, she would most likely want to go into something very specific: pediatric GI. Her internal debates, one would imagine, would go something like this: waste another five years of my life learning other types of surgeries to eventually get to begin doing fellowships in something I love. Five years. Five years of surgeries on adults. Five years where, yes, she would learn some very important things that would make her a better doctor, but also a lot of things that have no bearing on her future dreams.
I would consider anyone entering the medical field to be an expert at appreciating delayed gratification. But as my friends and I begin to plan out the rest of our lives, it sometimes seems like medicine is asking almost too much from us.
Blasphemy, I know. I've already spent hundreds of hours preparing for tests that I promptly forgot all the answers to. I've delayed seeing my own physicians--sometimes for months--in order to never miss a day of clerkship. I've stopped exercising and my diet consists of, and I am not kidding, microwavable popcorn, cheese sticks, and diet coke. Medicine has already asked a lot of us.
For me, my choice is easy: I've always felt strongly about family medicine, and as it turns out, you see a lot of psych patients in primary care settings. Family medicine: where you see everything and the residency program is only three years.
But for my friend Annette, her decision between surgery, pediatrics, and pediatric GI surgery has to take into account how much of her life she wants to live inside of a hospital.
Mar 22, 2014
Stereotypes in Medicine
It’s unfortunate that I want to go into family medicine,
because I think the stereotypes about family practitioners are often times
nonsensical. But I suppose it’s also good that both of my parents are kind,
friendly surgeons, so stereotypes about medicine’s specialties don’t really hold
true for me and my family.
So surgery often gets stereotyped as being full of jerks.
And while I think there are a lot of surgeons who seem to have an unnecessary
and occasionally dangerously elevated sense of self-worth, you find that in
other specialties, too, so I don’t think it’s terribly accurate.
Internal medicine people are obnoxious. It’s like they’ve
convinced themselves that what they are doing is interesting, even though
they’re stuck in a hospital all day dealing with dying people.
I want to say people going into radiology, ophthalmology,
and dermatology are all terrible people who are in it for the money instead of really helping people. But that’s not
true. And everybody’s idea of help is different. I don’t know why they’re
interested in their fields, but technically, someone’s got to do it.
Emergency Medicine is full of hipsters. I don’t know how
this happened, but it’s pretty accurate. People who are hipsters, people with
ADHD, and people who get bored easily. As for their personalities, they’ve got
their jerks and their saints, too.
Psychiatrists are indeed
crazy. But I think that’s because if you have a mental illness yourself,
dealing with medical students and physicians in other fields gets incredibly taxing. If I hear one more
person reduce major depression to a simple affair that people should be able to
handle without medicine, I may start applying to psychiatry residencies right
then and there.
Neurology is full of people who are more emotionally stable
than psychiatrists, but are still very, very weird. But understandably so. Like
more professional psychiatrists. Or just more stuffy.
I like pediatricians. But I wouldn’t say they’re the nicest
people in the world. Kids are just more tolerable than most other patient
populations, so it’s easier for them to look happier while they work. Whether
they are or not, nobody knows.
Obstetricians and Gynecologists are exactly like surgeons.
Who will occasionally smile at patients because their patients are neonates.
And that pretty much covers it. Does this effect what I want
to go into? Not really. It just makes me louder about defending my choice to go
into family medicine, which most people seem to think is incredibly boring, despite
the fact that, to me at least, it seems almost as exciting as emergency
medicine (when you remove trauma cases) while also including continuity of
care.
And to me at least, being a doctor means being a family
physician. All other fields just add complexity—necessary or not—to the medical
field.
Feb 24, 2014
Diagnosing One's Identity
I have started my psychiatry clerkship and I think I'm in love.
The staff is nice, funny, accommodating, kind. The physicians are crazy in their own way. The patients, well, the patients are all fascinating--there's something so complex about mental illnesses that makes it hard to reduce any one person to simply medicine alone.
And yet, with my patients, I feel like I keep reducing them to their diagnoses.
We are always told that patients are people--that we are treating them, not their illness. But with mental problems, the person is their illness because, well.... hmmm....
What is identity? It is the way we interact with our environment. It is our behavior. It is our thoughts, are consciousness. It is who we see ourselves as. It's what comes to your mind when you're asked to define yourself. Throughout college I told people I was "biracial, bisexual, and bipolar," because 1) I liked the way it sounded and 2) it seemed to partially capture the fact that my entire life I've seen myself as someone stuck in a huge gray area between the black and white poles of the various identities constructed by society. Definitively nothing, unquestionably everything: Elora Kathryn Apantaku.
But back to psychiatry and patients and their identities. I didn't realize how chronic most psychiatric disorders were. A lot of the older patients--in their fifties and sixties--a lot of them have been suffering from these illnesses--manic depression, major depression, schizophrenia--for decades. Their lives are so strongly influenced by their diseases... and although medication and therapy can help them stay out of the psych ward, their presence on the floor argues that they are doomed to continually function in a way that is maladaptive--either to their family, their friends, or to society.
The staff is nice, funny, accommodating, kind. The physicians are crazy in their own way. The patients, well, the patients are all fascinating--there's something so complex about mental illnesses that makes it hard to reduce any one person to simply medicine alone.
And yet, with my patients, I feel like I keep reducing them to their diagnoses.
We are always told that patients are people--that we are treating them, not their illness. But with mental problems, the person is their illness because, well.... hmmm....
What is identity? It is the way we interact with our environment. It is our behavior. It is our thoughts, are consciousness. It is who we see ourselves as. It's what comes to your mind when you're asked to define yourself. Throughout college I told people I was "biracial, bisexual, and bipolar," because 1) I liked the way it sounded and 2) it seemed to partially capture the fact that my entire life I've seen myself as someone stuck in a huge gray area between the black and white poles of the various identities constructed by society. Definitively nothing, unquestionably everything: Elora Kathryn Apantaku.
But back to psychiatry and patients and their identities. I didn't realize how chronic most psychiatric disorders were. A lot of the older patients--in their fifties and sixties--a lot of them have been suffering from these illnesses--manic depression, major depression, schizophrenia--for decades. Their lives are so strongly influenced by their diseases... and although medication and therapy can help them stay out of the psych ward, their presence on the floor argues that they are doomed to continually function in a way that is maladaptive--either to their family, their friends, or to society.
Feb 20, 2014
The Barometric Mind
I woke up this morning around 5:30, very briefly--thirty seconds maybe--because it was raining, and although the sound of rain beating on my apartment's giant windows overlooking the South Loop is usually really calming, the water dripping through my roof, through my ceiling, and onto my already stained carpet is quite distressing. But I didn't stay awake because at this point, a stained carpet is very low on my list of worries.
I'm thinking about away rotations and my grades and how to make myself look good for residencies. Am I forgetting paperwork? Probably. Where should I go next year? Do I want to go to Maine? Stay with my sister? Or should I go somewhere I've never been before, working in a hospital in Mississippi all by myself. Do I want to do family medicine rotations or psychiatric ones? These are the things I've been worrying about, but I recognize that my worries are not really important, just bothersome.
The patients in the psych ward, now their worries are real. Your family can't tolerate your manic outbursts anymore so they have you admitted--you promise to adhere to your medications from now on, but your family doesn't trust you any longer so now you don't have a home. Where do you go? In this already stressed out health care system, you run a real risk of becoming homeless--or as the hospital I'm working at calls it: undomiciled. That's a worry. Or let's say you're psychotic. Then the voices can give you a whole new set of things to worry about: "you're going to die as soon as you leave here" they might tell you, or "you need to be back on heroin again--that's the only thing that can help you, this anti-psychotic sh*t isn't helping and you and I both know it."
I arrive to the inpatient psych floor at 9:30. One of my patients, on the spectrum of schizophrenic to bipolar, is standing in the hallway, leaning against a wall. She looks terrible. "Good morning Miss [HIPPA compliant], you look tired, did you sleep well?" She says no. I stand next to her for a good fifteen seconds, waiting for her to elaborate, but she does not, so I slowly walk away, looking back at her as if she'll suddenly want to tell me more. Later, when I follow the doctor around like her own personal shadow, we stop by to see my patient. "This morning the nurses said you were banging against the wall and screaming, why was that?" My patient answers back something about "the voices" which I was almost positive had been alleviated by her sudden acceptance of her anti-psychotic meds.
Another patient, depressive with psychotic features, also has a similar complaint. The medications had helped reduce the voices to whispers, muttering always, no longer commanding. But this morning, they woke her up again, yelling at her. She looks tired today--much more so than yesterday.
I am a scientist--but I am a bad one. For me, personal anecdotal evidence is much more powerful than studies that have thousands of patients arranged into double blind groups and blah blah blah.... This is why when I think of sickle cell disease--how my dad's a carrier, my mom's not, but yet all three of their daughters have the trait--I think that there's more than coincidence going on with how it's inherited--either magic or some genetic translocation oddities.
Which is why I know believe that weather can make you psychotic. Two patients woke up in the middle of the night, around the time I woke up freaking out about the rain, and were brought back to their presenting level of psychosis. Maybe the pressure drop affected the neurotransmitters as much as it affected the forecast.
Just a silly, crazy, insane thought.
I'm thinking about away rotations and my grades and how to make myself look good for residencies. Am I forgetting paperwork? Probably. Where should I go next year? Do I want to go to Maine? Stay with my sister? Or should I go somewhere I've never been before, working in a hospital in Mississippi all by myself. Do I want to do family medicine rotations or psychiatric ones? These are the things I've been worrying about, but I recognize that my worries are not really important, just bothersome.
The patients in the psych ward, now their worries are real. Your family can't tolerate your manic outbursts anymore so they have you admitted--you promise to adhere to your medications from now on, but your family doesn't trust you any longer so now you don't have a home. Where do you go? In this already stressed out health care system, you run a real risk of becoming homeless--or as the hospital I'm working at calls it: undomiciled. That's a worry. Or let's say you're psychotic. Then the voices can give you a whole new set of things to worry about: "you're going to die as soon as you leave here" they might tell you, or "you need to be back on heroin again--that's the only thing that can help you, this anti-psychotic sh*t isn't helping and you and I both know it."
I arrive to the inpatient psych floor at 9:30. One of my patients, on the spectrum of schizophrenic to bipolar, is standing in the hallway, leaning against a wall. She looks terrible. "Good morning Miss [HIPPA compliant], you look tired, did you sleep well?" She says no. I stand next to her for a good fifteen seconds, waiting for her to elaborate, but she does not, so I slowly walk away, looking back at her as if she'll suddenly want to tell me more. Later, when I follow the doctor around like her own personal shadow, we stop by to see my patient. "This morning the nurses said you were banging against the wall and screaming, why was that?" My patient answers back something about "the voices" which I was almost positive had been alleviated by her sudden acceptance of her anti-psychotic meds.
Another patient, depressive with psychotic features, also has a similar complaint. The medications had helped reduce the voices to whispers, muttering always, no longer commanding. But this morning, they woke her up again, yelling at her. She looks tired today--much more so than yesterday.
I am a scientist--but I am a bad one. For me, personal anecdotal evidence is much more powerful than studies that have thousands of patients arranged into double blind groups and blah blah blah.... This is why when I think of sickle cell disease--how my dad's a carrier, my mom's not, but yet all three of their daughters have the trait--I think that there's more than coincidence going on with how it's inherited--either magic or some genetic translocation oddities.
Which is why I know believe that weather can make you psychotic. Two patients woke up in the middle of the night, around the time I woke up freaking out about the rain, and were brought back to their presenting level of psychosis. Maybe the pressure drop affected the neurotransmitters as much as it affected the forecast.
Just a silly, crazy, insane thought.
Feb 11, 2014
Death, Dying, and a Defense Mechanism
So our school often has us write silly things to talk about our feelings. Which is dumb, since I no longer have any (a lie, but I don't seem to have any today). But sometimes they help me write random things for this blog, like Fixed and Dilated. Anyway, here was the prompt:
And here was my response:
Write about
your interactions with a patient who died or was very ill. What sources of
inspiration did you find in caring for this patient? How did your team manage
the patient’s and the family’s hope
in the face of a poor prognosis or outcome?
And here was my response:
I’ve taken care of a lot of patients that later died.
And now that I think about it: I didn’t do anything special
to comfort any single one of them. Because death is a terrible thing, and I
wouldn’t want to share my last few days on earth being “comforted” by a medical
student. So no, I haven’t actually jumped up to volunteer to annoy someone and
their beleaguered family in their last days of life.
[Also, we haven’t been taught how to deal with death, right? Because that wasn’t a
lecture and I’m not comfortable dealing with it now.]
But back to me thinking about how I’d want to die…. if I’m still mentally alert, I think I’d want two
things: as many pain meds and anti-anxiolytics as I can tolerate and to be
surrounded by my closest friends and all
my living family members. I also wouldn’t want to be in a frickin’ hospital,
but the odds are in favor of that so I guess I should start preparing now. One
could make the argument that as you get older, and if you’re dying of a slowly
progressive disease, your psychology changes to accept death, which is
something I haven’t had to do yet as a “healthy” twenty-something. But I think
that’s dumb. I had a patient tell me he was superman, that he was going to
somehow defeat/prolong his battle with metastatic prostate cancer—and then I
sat outside his hospital room and listened to his freshly-minted widow cry when
he died five weeks later.
And I did nothing.
I could only find comfort in the fact that I had at one
time spent a good thirty minutes with the patient explaining why we were
holding him in the hospital overnight those five weeks earlier. But now I’m not
sure if my need to talk through disease processes and hospital operations to
the patients and their families is my way of comforting or just the defense
mechanism of intellectualization. Because I have nothing to say. You’re going
to die. I wish I could do something. I wish we could keep chatting about your
interracial grandchildren, or about how pretty my earrings are, or clarifying that
you’re at MOUNT SINAI HOSPITAL not in the KOREAN WAR, but I can’t stop your
death. I can hold your hand. I can call your children. I can maintain eye
contact. And I can tell you as much as I know. Which isn’t a lot.
Subscribe to:
Comments (Atom)